Most people have accepted a life of “a little overweight” or have been told by today’s standards they are considered “Obese”. Most people tend to disregard these and just acquiesce to a new normal where everyone has some form of weight struggles, and simply accepts this new normal and the only answer is to “size up.”
The other problem is the socialization through media, medicine, and processed food marketing, that this is really the new normal….that everyone is a few sizes bigger these days, and we see whole towns of overweight and obese people singing, dancing in the streets or the offices where they work, wearing colorful outfits, and behind the scenes, taking life and health threating injections.
All this at the cost of billions of dollars of advertising to convince the world that this is normal, and any discussion to the contrary, we are told, is body shaming.
SOMEONE HAS TO SAY…..THIS IS NOT OKAY.
So let’s look at some of the real world health risks directly coming from being OVERWEIGHT & OBESE:
1. Metabolic & Endocrine
- Type 2 Diabetes
- Insulin resistance / prediabetes
- Metabolic syndrome (high blood pressure, high blood sugar, abnormal cholesterol, excess abdominal fat)
2. Cardiovascular
- High blood pressure (hypertension)
- High cholesterol and triglycerides (dyslipidemia)
- Early signs of atherosclerosis (fatty buildup in arteries)
3. Respiratory & Sleep
- Obstructive sleep apnea (pauses in breathing during sleep)
- Asthma or worsened asthma symptoms
4. Musculoskeletal
- Joint pain and musculoskeletal strain
- Slipped capital femoral epiphysis (SCFE) (hip problem)
- Blount disease (growth disorder of the shin bone)
5. Gastrointestinal & Hormonal
- Nonalcoholic fatty liver disease (NAFLD) (fat buildup in liver)
- Gallstones
- Polycystic ovary syndrome (PCOS) beginning in adolescent girls
6. Psychological & Social
- Low self-esteem and body dissatisfaction
- Bullying and social stigma
- Anxiety and depression
- Eating disorders (binge eating, restrictive cycles)
All of these were once categorized as “ADULT ONSET”, but believe it or not, THESE COME FROM 2024 SOURCES like World Health Organization, UNICEF, NCD-RisC, CDC, and many more US Public Health sources…..
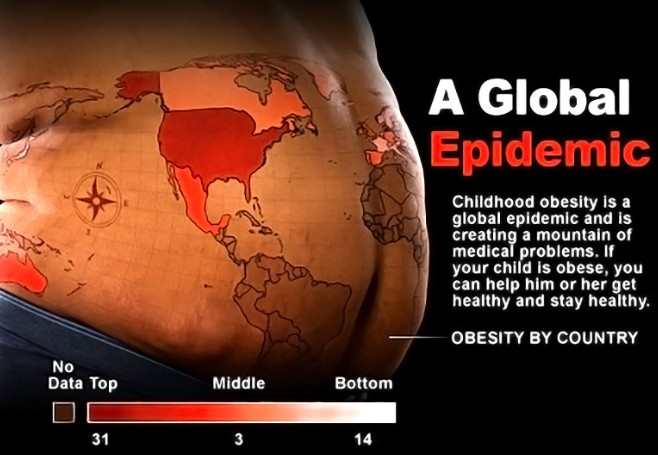
Frighteningly enough, the above 6 issues of poor metabolic health did not come from any studies of adults. ALL OF THESE ARE THE SUMMARIZED HEALTH DEFICITS AND MEDICAL ISSUES IN CHLDREN AROUND THE WORLD…….THIS IS THE DATA BEHIND CHILDHOOD OBESITY.
| Metric | Value / Estimate | Notes |
|---|
| Children under 5 over-weight | ~35 million | Globally in 2024, more than 35 million children under age 5 were estimated to be overweight. World Health Organization |
| Children & adolescents (age 5-19) overweight (includes obesity) | ~391 million | As of ~2022, about 1 in 5 children/adolescents are overweight. WHO Test CMS+2UNICEF DATA+2 |
| Obesity (severe form) among the 5-19 age group | ~160 million | In 2022, about 8% of children/adolescents in that age group were obese. WHO Test CMS+2UNICEF DATA+2 |
| Overweight vs Underweight shift | Obesity now exceeds underweight among school-age children/adolescents globally in most regions | In 2025 UNICEF reports that obesity among ages 5-19 has surpassed underweight in all regions except sub-Saharan Africa & South Asia. Earlier, underweight was more common globally. |

HAVE YOU HEARD WHAT THE “STANDARD OF CARE” IS FOR OUR CHILDREN?
To fully appreciate how frightening this is, you have to wrap your head around the FACT, that children are coming out of the womb OBESE, and DIABETIC….WHY?
BECAUSE CHANCES ARE THE METABOLIC POOR HEALTH OF THE MOTHER IS BEING DIRECTLY FED TO THE CHILD IN THE WOMB……..so let me re-iterate, this was only considered “adult onset” diseases at the beginning of most of our lives, and now children are being born with all the complications of OVERWEIGHT & OBESE.
The other point of “appreciation” according to these studies is that in today’s world, it will not be uncommon for parent to outlive their OVERWEIGHT & OBESE children as a direct result of these illnesses so early in life.
Here is the official paper trail on “standard of care” for childhood obesity:
1. Lifestyle & Behavioral Interventions (first-line)
- Nutrition counseling → balanced diet, portion control, reduced sugary drinks/snacks
- Physical activity → at least 60 minutes/day of moderate-to-vigorous activity
- Screen time limits → replacing sedentary time with active play
- Family-based programs → involve parents in modeling healthy behaviors
- Behavioral therapy → goal setting, food diaries, reward systems, cognitive-behavioral therapy (CBT)
- In My Opinion – Nutrition Counseling is the only SMART thing on this entire list – none of the illness has to do with activity, screens, modeled behavior, or their own behavior. This is strictly from the evolution of our processed foods, as well as the strong influence of pharmaceutical companies socializing the idea of unsafe injections to stop a symptom rather than simply whole foods to cure a problem.
2. Medical Interventions (for severe obesity, usually ≥ age 12)
- Medications approved for adolescents:
- Orlistat (age ≥12) → reduces fat absorption
- Liraglutide (Saxenda) and semaglutide (Wegovy) (age ≥12) → GLP-1 receptor agonists that help with appetite regulation and weight loss
- Phentermine/topiramate ER (age ≥12 in some cases, depending on approval status)
- In My Opinion – WAIT…..WHAT!!!! These injections….when marketed for diabetes, are limited in the duration they can be taken because of long term side effects and damage to other organs and risks associated with them, but the IDENTICAL injection, when marketed under different labels for weight loss….can go on indefinitely…..with the same lasting, irreversible damage…..ARE WE SURE THIS SHOULD BE ON THE LIST……There is no easy way out like a shot….there is no shortcut to LONGEVITY.
3. Surgical Options (for severe obesity, usually ≥ age 13–14)
- Bariatric surgery (e.g., gastric sleeve, gastric bypass) considered only for adolescents with:
- BMI ≥ 120% of the 95th percentile (or BMI ≥35 with serious health problems)
- After failure of lifestyle and medical treatment
- Requires extensive psychological and medical evaluation before approval
- In My Opinion – ARE YOU KIDDING ME….for children? Is anyone asking why? These surgeries CANNOT BE UNDONE….Almost all of the adults we work with that have had this surgery have regained the weight and more anywhere between 10 – 14 months, leaving them with severe physical and psychological limitations from the surgery, as well as the return of illness from THE METABOLIC SYNDROME…..and this is approved for children at an age when their biggest concern should be if their voice has changed yet.
4. Supportive Care
- Multidisciplinary obesity clinics → pediatricians, dietitians, psychologists, exercise specialists
- Treatment of comorbidities → medications for high blood pressure, insulin resistance, or high cholesterol if lifestyle alone isn’t enough
- In My Opinion – This also can be eliminated if, from the beginning we educate people on the NATURAL CHEMISTRY AND ACTIONS OF THE HUMAN BODY – For every action there is an equal and opposite reaction…..this is SO true when it comes to what we genetically modify in the foods that are produced for profits rather than people, and when we medicate for symptoms created by processed foods, rather than EDUCATE patients to stop eating those foods, and to not see pharmaceutical options as viable.
THERE IS HOPE.
If you or a loved one would like to have a FREE, confidential discussion to see what strategy could help you, your loved one, and most importantly your children, just GO HERE, and click the green “SCHEDULE TIME” button to discover a new beginning of metabolic health.